Robotic assisted minimally invasive surgery has changed the face of surgery. The use of robotic aids in surgery can be traced back to the mid-1980s, when robotic systems were used to create precise incisions, cuts and drills. From the late 1990s onwards, robotic surgery has taken a leap forward with the FDA’s clinical approval of systems such as daVinci. These systems consist of a telemanipulator, allowing a surgeon to control mechanical arms and surgical instruments from afar, removing thus the constraint of having the surgeon in the surgery room. Other robotic systems are attached to the patient’s body and allow navigation of instrument through them (NeuroMate, approved by the FDA in 1997). The robotic system moves with the patient body as one, allowing surgeons to operate in a stable environment. Robotic surgery holds many other advantages over traditional open surgery such as shorter recovery time, lower risk of infection and higher precision, to name a few.
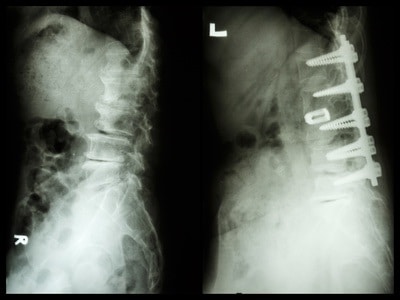
When precision in operation is demanded, surgeon’s dexterity cannot be a compromise. In neurological surgery (brain or spine) misplaced screws account for 10% of cases, which might cause permanent nerve damage or cerebrospinal fluid leakage. In contrast, robotic guidance systems have been shown to produce near zero cases of misplacement. In spine surgery, placement of screws need to be accurate to less than 1mm. This accuracy is achievable by trained surgeons; however, it can become even more accurate when a robotic system compensates for involuntary and normal patient displacement.
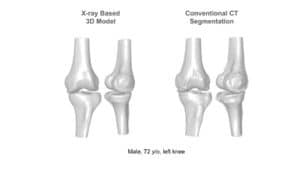
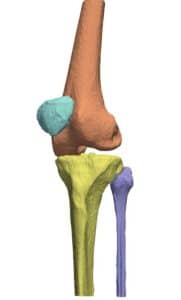
Accurate planning of screw insertion is key to properly guide the robot to the desired trajectory for screw insertion, electrode planting, or biopsy: with tissues crowded in nerves and blood vessels, robotic systems rely on visual information acquired preoperatively by modalities such as CT. Different modalities can be used in preoperative imaging, producing planar and volumetric data. In the planning stage of the operation, the three dimensional shape of spinal bones are crucial information for determining the insertion trajectory. For this end, planar X-ray and volumetric or planar CT images are registered to give rise to a 3D CAD model of the designated site.
Registration between images of different modalities involves essentially aligning them so that each points correspond to the same position in a new coordinate system. Strategies for semi-automatic image registration include calculation of the rigid transformation parameters required to manually change a set of point in one image to its corresponding set of points in the other image. Automatic means of registration are more advanced and rely on extracting sets of salient markers in one image e.g. corners, ridges and blobs, and automatically find their correspondence in the other image.
Statistical methods are commonly employed in the point matching procedure, since generally the number of features extracted in each images does not match. A robust and fast way to perform such statistically-based matching is to use the Random Sample Consensus (RANSAC) method, which draws a sample of feature points (or their representation in another coordinate system) and fits it to the model of allowed transformations. A collection of possible transformation given by RANSAC can be scored and further analyzed such that the chosen transformation parameters from one image to the next is robust with regards to the choice of sampled features.
Multimodal registration is an essential first step toward a full 3D reconstruction from preoperatively acquired images. The resulting 3D CAD model is a valuable tool in the planning of screw insertion procedure and reduces the need for additional imaging steps to assess bone and other organs. Registration can also be performed between preoperative and intraoperative imaging.
Precise registration from multimodal imaging system has long been performed by image processing engineers at RSIP Vision. Advanced algorithms developed and utilized by RSIP Vision are currently used in registration of the vascular tree in retina images, cardiac fluoroscopy and many more practical applications.
Accurate planning of screw insertion is key to properly guide the robot to the desired trajectory for screw insertion, electrode planting, or biopsy: with tissues crowded in nerves and blood vessels, robotic systems rely on visual information acquired preoperatively by modalities such as CT. Different modalities can be used in preoperative imaging, producing planar and volumetric data. In the planning stage of the operation, the three dimensional shape of spinal bones are crucial information for determining the insertion trajectory. For this end, planar X-ray and volumetric or planar CT images are registered to give rise to a 3D CAD model of the designated site.
Registration between images of different modalities involves essentially aligning them so that each points correspond to the same position in a new coordinate system. Strategies for semi-automatic image registration include calculation of the rigid transformation parameters required to manually change a set of point in one image to its corresponding set of points in the other image. Automatic means of registration are more advanced and rely on extracting sets of salient markers in one image e.g. corners, ridges and blobs, and automatically find their correspondence in the other image.
Statistical methods are commonly employed in the point matching procedure, since generally the number of features extracted in each images does not match. A robust and fast way to perform such statistically-based matching is to use the Random Sample Consensus (RANSAC) method, which draws a sample of feature points (or their representation in another coordinate system) and fits it to the model of allowed transformations. A collection of possible transformation given by RANSAC can be scored and further analyzed such that the chosen transformation parameters from one image to the next is robust with regards to the choice of sampled features.
Multimodal registration is an essential first step toward a full 3D reconstruction from preoperatively acquired images. The resulting 3D CAD model is a valuable tool in the planning of screw insertion procedure and reduces the need for additional imaging steps to assess bone and other organs. Registration can also be performed between preoperative and intraoperative imaging.
Precise registration from multimodal imaging system has long been performed by image processing engineers at RSIP Vision. Advanced algorithms developed and utilized by RSIP Vision are currently used in registration of the vascular tree in retina images, cardiac fluoroscopy and many more practical applications.
 Orthopedics
Orthopedics